Software Can Cut Costs for Health Insurers — But Watch Out for TCO Overruns


Editor's note: Olga Vinichuk, Insurance IT Consultant at ScienceSoft, shares cost-saving workflow automation features and ways to optimize software-related expenses in health insurance. For the purpose of this interview, the broad category of operational costs is limited to personnel and IT spending. The interview is led by Stacy Dubovik, a financial technology researcher.
Software Is Both a Cost Saver and a Cost Driver. How Do You Maximize the Former?
SD (Stacy Dubovik): In your experience, where do insurers lose the most money when it comes to operations?
OV (Olga Vinichuk): I’d say inflated personnel costs stemming from tedious manual routines and the use of outdated technology.
One obvious pain point is the lack of proper data processing automation and software integrations. Without automation (or with it, if it’s poorly done), employees end up wasting hours every day on consolidation, validation, and reconciling of data across multiple disparate systems. This results in low staff productivity and delays and sometimes pushes carriers to hire more employees, driving even higher overheads. I’ve heard of a case when a health insurance agency gradually grew an enormous pool of agents to handle mundane application processing, customer onboarding, and servicing tasks just because its CRM didn’t have adequate automation features.
SD: Is implementing process automation or raising its degree the best way to improve operations?
OV: Automation is indeed a proven strategy for reducing operational expenses without cutting staff. However, its efficiency directly depends on the maturity of a health payer’s business processes. The dependence is best seen in custom software, which usually inherits the logic of a company’s workflows completely, with all its friction. Tangled and redundant operations complicate software logic and may hamper its performance, not to mention the extended time and cost required to code it.
To make the most of automation, you should first optimize your business processes and make them leaner. As an example, one of my clients managed to remove unnecessary steps from its claim processing workflows before automating. This helped the company increase the degree of automation and reduce software development costs.
SD: What gains can health payers expect from automating their servicing tasks?
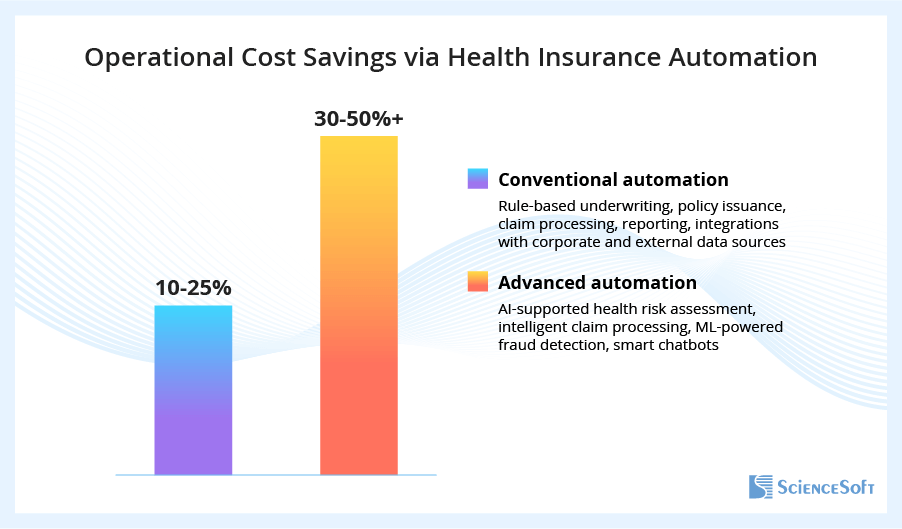
OV: This depends on the scope of automation and the applied technology. From my experience, it’s absolutely possible for a midsize health payer to achieve 10–25% cost savings via conventional automation across major operational areas like underwriting, claim processing, and reporting. AI-powered automation can cut expenses across these areas by 30–50%+.
SD: All right, so how much should you invest in automation before it becomes too much? How do we make sure the fix doesn’t cost more than the problem used to?
OV: Cost savings brought by automation definitely shouldn’t be measured in isolation from the TCO of IT. The process of cost-benefit analysis is quite straightforward.
First, you need to estimate financial gains. A common approach is to determine the number of working hours or FTEs freed by automating a task and multiply them by the number of employee payouts for the equivalent period.
Then, estimate the TCO for the automation solution (custom-built or off-the-shelf software, depending on your choice). For custom development, consider initial investments in solution design, engineering, and integration. To estimate them, you need to know the scope of project tasks, FTEs and timelines to complete them, and resource prices (if you opt for outsourced development, your vendor should provide a detailed estimate — you can read more about this practice and check estimate examples here).
For ready-made software, consider at least five-year licensing and subscription costs, as well as customization and integration expenses.
In both cases, make sure to include long-term maintenance and support costs, user training expenses, and compliance-associated costs (for example, to establish and maintain HIPAA compliance if your software will process PHI).
Finally, compare the TCO against the gains to figure out whether your planned software is feasible.
I always warn my health insurance clients that preliminary cost estimates for custom projects are rarely 100% accurate, but it’s not a barrier to precise TCO evaluation. For example, most of the companies I worked with requested viable software changes midway, which increased the development budget by 5–10%. Knowing this, I apply a 1.1x correction to the initial TCO to get a more realistic cost-benefit ratio. I also add a correction coefficient to account for the costs of addressing unforeseen risks like regulatory changes.
What to Automate First to Save the Most
SD: Let’s talk strategy. Where should a health insurer start on its way to software automation? Can you — and should you — automate everything?
OV: Complete digital transformation brings cost savings across the entire health insurance value chain. But, in my practice, insurers who struggle with high operational expenses often have tight budgets for their digital initiatives and, as such, rarely start with large-scale overhauls.
Many of my health insurance clients see high-impact transformations across particular service areas like underwriting or claims as the most desirable outcome. The strategy is economically reasonable: it usually targets the most cost-intensive workflows and brings impressive savings. Plus, it’s relatively quick to plan and implement. Achieving a fast ROI on IT investments will justify the financing of further digital projects and may secure a bigger budget due to optimized operational expenses.
Your targeted transformation strategy will involve either implementing new software or modernizing your current solution. Despite widespread belief, switching to a new tool is often cheaper than upgrading a heritage system. The scope of revamp may vary from adding new features to complete rearchitecting, and its costs may be significant in case of serious system rebuilds. When my client wants a revamp, I involve ScienceSoft’s architects to audit the company’s software and tell us if modernizing it would be as feasible as replacing it.
SD: Sure, every health payer is unique. But from your experience, what automation features have the biggest impact on health insurers’ bottom lines?
OV: I would say invest in integrating your underwriting system with customer-facing apps (say, your website or mobile app), CRM, and providers’ EHRs to automate the aggregation of insurance applications and health risk data. Automated risk data capture alone saves health insurers $100–$800 per application.
AI-supported health risk assessment can bring a 10–50%+ reduction in underwriting costs via enhanced risk profiling and minimized losses associated with inadequate risk pricing. You’ll need tailored large language models (LLM) and deep learning algorithms to enable this feature. LLMs auto-extract and summarize risk data from application documents and EHRs, providing your underwriters with decision-ready data in minutes. LLMs can also validate the data against EHRs to assure its accuracy and completeness. Deep learning engines then score health risks, instantly produce tailored quotes for low-risk applicants (which are likely up to 90% of all applicants), and flag specific medical conditions that require manual assessment. I shared insights into compliant and budget-friendly ways to automate health risk evaluation in my recent guide.
By launching automated processing of claim evidence, some of my health insurance clients achieved up to 70% cost savings across their most data-intensive tasks. Intelligent text, image, and video analysis algorithms trained on your proprietary data and healthcare specifics only need minutes to recognize and interpret all sorts of multi-format claim evidence, from medical statements to 3D MRI. They can further group claims by issue type and triage them for settlement according to your internal policies.
Same as in the case of risk assessment, consider integrating your claim software with healthcare providers’ EHRs for evidence auto-validation.
Automated fraud detection is widely applied in claim evidence processing, but let’s talk about it separately as it has tremendous impact on health payers’ bottom lines.
At ScienceSoft, we’ve recently dealt with developing machine learning (ML) algorithms for dental insurance fraud detection. Based on my estimates, ML-supported recognition of fraudulent claims may help large payers reduce annual fraud detection and investigation costs by $1M+ and cut the losses associated with illegitimate and inflated payouts by up to 90%. The benefits are mainly attributed to ML’s ability to spot forgery patterns that are invisible both to the human eye and to conventional automation tools. So yes, it means that you need specifically machine learning to get the same results.
The good news is that you won’t have to invest millions. In ScienceSoft’s projects, we managed to deliver standalone intelligent components for risk assessment, claim processing, and fraud detection within the budget of $150,000–$300,000.
Cutting the Cost of Heritage and New Systems: Tech Stack, Sourcing, and Beyond
SD: Let’s move on to IT costs. Taking a midsize health payer with a more or less mature software system, how do you optimize its ongoing maintenance costs?
OV: Midsize health payers can cut IT expenses by moving their business-critical systems from on-premises or hybrid hosting to a cloud-only infrastructure. This step eliminates the costs of hardware maintenance, reduces infrastructure management expenses thanks to automated cloud controls, and lowers software evolution costs due to streamlined development and deployment operations. Major cloud providers like Microsoft and Amazon offer on-demand cloud computing and consumption-based pricing, meaning you can quickly scale processing capacity when needed while paying only for the actually used resources.
If you’re already in the cloud, there’s an opportunity to rightsize cloud resources. My colleagues from ICT use Amazon CloudWatch and Azure Monitor to continuously monitor cloud performance and identify unused and underutilized cloud resources. By downsizing instances with consistently low CPU and memory usage, the team saves each client up to $600 per instance monthly. Major health insurance SaaS products (e.g., Microsoft Cloud for Healthcare, which offers health payer modules) provide cloud resource auto-rightsizing capabilities.
Routine maintenance workflows like infrastructure and app monitoring, backup and recovery, and storage provisioning are good candidates for automation. From my experience, employing automated tools can bring health insurers a 30–45% cost reduction across these tasks.
Outsourcing non-core IT functions like the employee help desk is another strong cost-saving strategy. My insurance clients who trusted their Tier 1 staff support tasks to third-party vendors reported up to a 40% decrease in help desk costs.
SD: Ready-made health insurance software is widely believed to be more budget-friendly compared to custom development. Should payers with non-specific needs resort to off-the-shelf products by default?
OV: Off-the-shelf tools require minimal upfront investments and may be a more budget-friendly option in the short term. However, you have to pay ongoing licensing fees and may end up investing more along the way to add integrations, additional users, or extra custom features. Eventually, you might find that the TCO of your pre-built solution exceeded the TCO for custom development.
Custom software offers everything that OOTB tools don’t but comes at a way higher upfront cost. Here, however, you pay off the biggest share of TCO at the door and bear minimal expenses down the road.
Let’s see what it means in practice. For example, Zipari, a provider of health insurance software products, may charge $100,000+ annually for its combined offer of a customer portal plus mobile app, excluding add-ons and integrations. From my experience, building a fully featured custom portal plus app may cost, on average, $220,000–$280,000, including integrations. The TCO is comparable already in the third year of use, and in the five-year perspective, a custom solution becomes more cost-effective.
SD: Then, how do you control costs and timelines in custom software engineering? We’ve all heard of nightmare projects that lasted years and led to nothing.
OV: My health insurance clients often worry that custom development will take years when they need to see the first results before the end of the current fiscal period. Releasing an MVP is a go-to way to quickly introduce core solution features and accelerate payback. In some of ScienceSoft’s Agile development projects, we managed to deliver an MVP of health insurance software in just three months.
As for the process controls, you will need strict scope management and proactive budget control to prevent scope creep and cost overrun, two frequent issues in Agile projects. Documenting the scope, exclusions, and potential extensions and mapping change requests against the scope documents helps avoid inflating tasks – and costs – while still leaving room for reasonable adjustments. Continuous monitoring of the budget variance will let you spot discrepancies between the actual vs. planned costs early and quickly take corrective measures.
To further reduce costs, consider established nearshore and offshore destinations, which offer 2–3x lower talent rates compared to the US. Commissioning development abroad typically saved my US clients 40–70% of overall project costs.
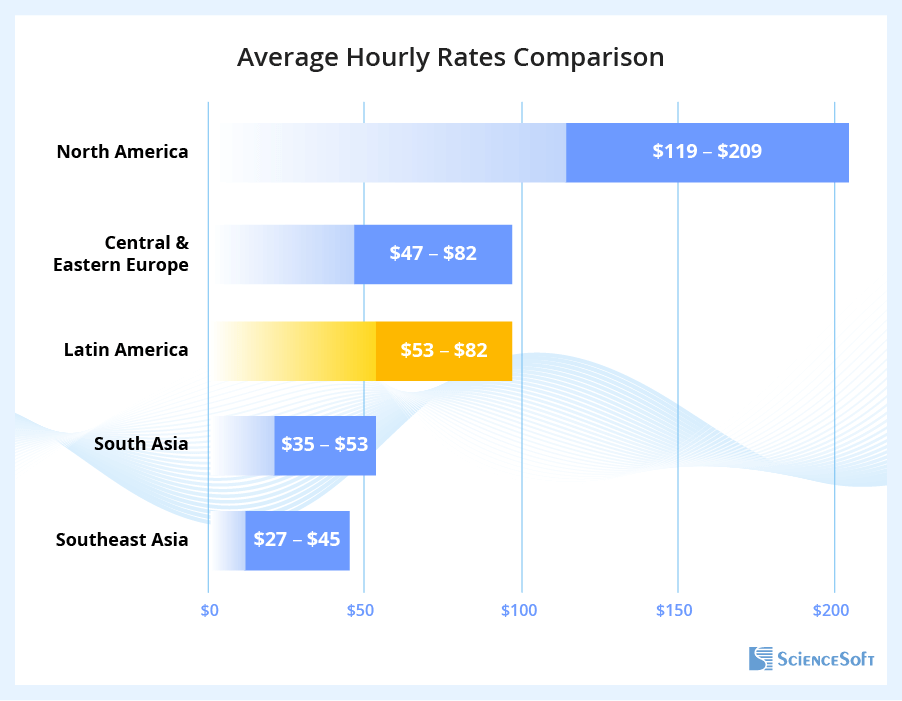
If you hesitate about the potential communication, delivery, or quality issues, prioritize software vendors with distributed capacities (e.g., consultants and PMs in the US, engineers in Europe or LATAM). Such vendors natively align with the US quality standards and business ethics. Also, make sure your vendor has experience with the US health insurance regulations (primarily HIPAA and NAIC) and is able to deliver legally compliant solutions.
If you need advice on development cost optimization options for your specific case, feel free to contact me or other consultants at ScienceSoft.