Harnessing PGHD for type 2 diabetes management: glucose level

Patient-generated health data (PGHD) can give both patients and physicians a reliable tool to support the Type 2 diabetes management. This data can include glucose level, blood pressure, medication intake, food and water consumption, and more. However, this article will focus on blood glucose, as diabetes patients are more motivated to regularly measure it.
Practically, these measurements serve patients only for self-management, while providers can collect PGHD, analyze it and achieve improved health outcomes. Let’s review some of them.
3 clinical outcomes of proper PGHD use
Permanent control over a patient's vitals – in our case, glucose – can offer caregivers the following benefits:
Timely updates of the treatment plan
As patients’ health status is constantly changing, providers need to have actual information about their chronic disease management course and be 100% sure the current treatment plan is working. The reasons to change the treatment plan can adjust to:
- Lifestyle changes (relocation, new physical activities or other)
- Changes in the patient’s body (insulin resistance increase, insulin secretion decrease in beta cells, infection)
- Influence of the parallel treatment (for example, if the patient takes sulfonamides affecting absorption, transport, metabolism and elimination of SU derivatives)
A glucose level increase or glucose surges may signal that treatment is to be changed.
Identification of negative trends
Diabetes is a disease for life, thus continuous measuring and processing of blood glucose data allows to determine both negative and positive trends in a patient’s health status. If the glucose level slowly rises with no changes to the treatment plan, hydration, nutrition and physical activities, a physician can recognize negative patterns and determine their triggers as soon as possible.
For example, not all Type 2 diabetes patients require the insulin therapy, as about 40% can treat their condition with an antidiabetic oral agent. Thus, if the patient takes only oral medicine, this lasting and progressive hyperglycemia can show that the day-to-day treatment doesn't help the patient effectively. In this case, the physician can change a medication, prescribe an additional insulin therapy to complement or even replace the oral drug.
Patient motivation
Last but not least outcome is a more effective patient engagement and motivation.
If a patient doesn’t share the measured glucose levels with their caregiver, then why should they keep records at all? During the appointment, a patient will, at best, offer their physicians to check a few recent measurements, daily or weekly.
On the flip side, if a patient knows that each new number will be recorded and analyzed for the sake of accurate diabetes treatment, they are motivated to measure their blood glucose more often and regularly note it down.
Moreover, PGHD allows motivating a patient for a more systematic care. If recent measurements highlight the need for an appointment or an HbA1c test to evaluate the overall trend, the patient can be notified about this need, possibly automatically.
Overriding PGHD skepticism
Every idea should tackle healthy doubts, so we have a few to review as well.
Noisy PGHD
There is a lot of noise in PGHD (e.g. wrong calibration, irregular measurements) and it is a reason to be skeptic about the clinical outcomes. However, raw data is often foggy and a little messy before you process it. We can rely on technology to clean it and prepare for further analysis. Besides, a physician uses PGHD insights for preliminary assessment of a patient’s health status, so it is always possible and even desirable to refer him or her to a lab to get a more detailed condition picture (if a patient takes up an HbA1c test).
Patient can handle PGHD without a doctor
Sure, patients can and should control their blood glucose, however, we should also remember the nature of the human mind. Our psychology works 24/7 to defend us from emotional traumas, and a chronic condition might end up being in the list of traumatic experiences. Consequently, some patients might completely give up on blood glucose monitoring, thinking that healthy behavior make the disease disappear for good.
Moreover, patients are not certified health specialists (well, not all of them, at least) trained to objectively identify negative trends and change their treatment plans accordingly.
Basics of PGHD implementation
Where to store data
Sorry, EHR, you’re out. Even if we talk about blood glucose inputs only, the volume of data is too massive to store it inside the EHR. We suggest integrating a separate storage that will be able to collect and keep the PGHD for years. Reports can be introduced into EHR as virtual tests, where not every measurement is recorded but a summary (surges up to 220 mg/dL in Apr or a trend of glucose level growth at 2-5 mg/dL a month).
How to analyze it
To ensure profound analytics, we need to take into account both old and new technologies. Some of the continuous glucose monitors (CGM) and instant finger-prick tests are able to connect with a patient’s mobile device via a specific application. However, when a patient’s insurance covers only cheaper or older meters, this connection is no longer an option. In this case a mobile application can also be a way out, as an individual can manually input his or her numbers and share them with a caregiver.
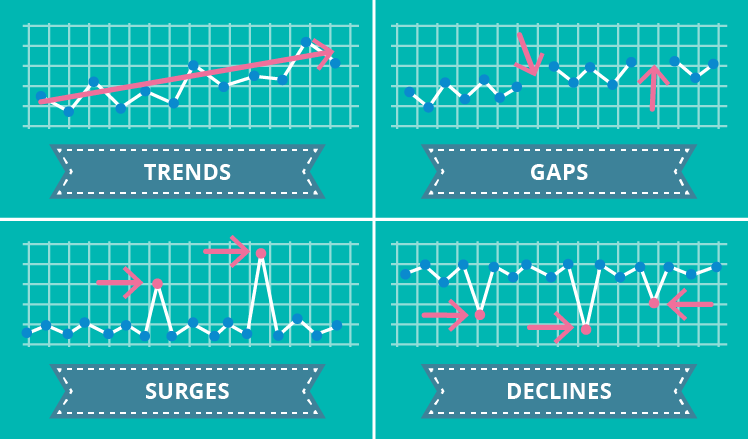
Now, if we have a monthly set of a patient’s measurements, we can already gain the following insights:
- Trends can show if the patient’s condition gets worse or better via the statistically calculated regression function visualized as an ascending or descending graph
- Gaps belong to noise, however, they can indicate a patient’s negligent attitude to glucose control
- Surges show glucose peaks and highlight if a patient consumes too much sugar or carbs, neglecting nutrition recommendations
- Declines are even more important than surges, as they mark high odds of hypoglycemia, which is especially dangerous during sleeping hours
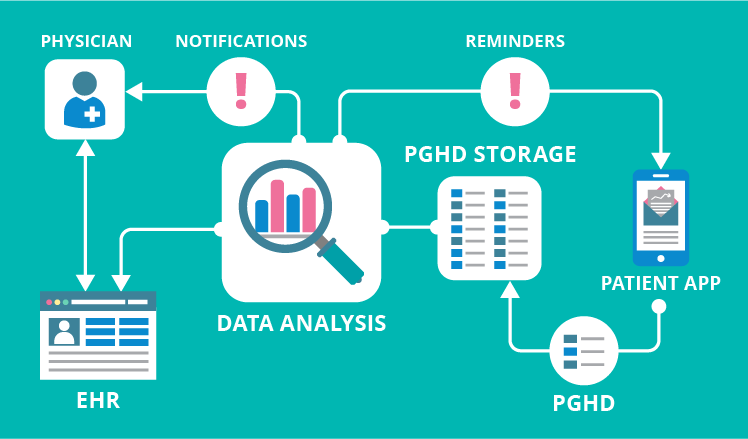
Enabling notifications
No one expects a physician would study tons of PGHD records and make conclusions. Instead, technology is here to notify a physician and / or patient in predefined cases (as illustrated in this online demo).
For example, if the trend graph is ascending, a physician can get a notification about that. If there are several gaps in measurements, a patient can get a reminder to check and input his or her numbers. Technically, notifications can reach their addressees through mobile app push notifications, via emails, text messages and other communication channels.
Summing all up
Woah, what a journey. What we want to say in this afterword is that PGHD is the type of data you have scattered across thousands of diverse patient devices. Sure, this information needs efforts to gather, clean, analyze and distribute it.
Yet disregarding the possibility of putting PGHD to use means ignoring the opportunity to improve diabetes care delivery. You are able to help diabetes patients stay in the zone of normal blood glucose numbers and never experience complications or exacerbations. So let’s do it and help them the best we can.
